Computer and Technology Enhanced Hypnotherapy and Psychotherapy.
A review of current and emerging technologies: 2008.
© Bill Frost 2008
Version History
- 31 Oct 2007 First draft finalised
- 19 Nov 2007 After initial reviews and edits
- 04 Feb 2008 Final revisions prior to publication
Contents
Background
For hundreds of thousands of years humankind has sought to change the way in which we think, feel and behave through external mechanisms. As our knowledge and technologies have evolved such mechanisms have included religion, music, recreational drugs and alcohol, psychotherapy, philosophical self-help, biofeedback, electrical convulsive therapy and psycho pharmacological medications.
With each new era of technological innovation we seem to experimentally apply those innovations to our own minds. The results are as varied as the individuals to which they are applied or adopted - what works for one person is seen as ineffective or even damaging by another person. Such is the nature of the human experience.
Now in the 21st Century our desire to change how we think and feel is as strong as ever, perhaps more so as more and more people come to have the expectation and belief that we should be able to control how we think and feel and behave. What has changed over the last few decades are the number of routes available to achieve that change and the ready availability of many of those routes with the advent of the personal computer and the internet.
Mechanisms that were once only available via specialists are now often freely available to anyone with access to a computer or phone - 24 hours a day, 7 days a week, 365 days per year. Changing how we think, feel and behave has almost become a religion in its own right. Commandments have become presuppositions, prophets have become self-help gurus.
Research Objective
The objective of this paper is to research the technological mechanisms that are currently available to the general public, psychotherapists and psychotherapy patients that directly assist in, or substantially enhance, the mind-change process. Up and coming emerging technological solutions on the horizon will also be given some consideration where there is a reasonable probability that those technologies will mature into viable commercial products. This paper primarily addresses technologies that can be utilised by psychotherapists that specialise in clinical hypnotherapy.
Acknowledgments
 I am both a psychotherapist and a technologist. I firmly believe in the power of technology and the power of many psychotherapeutic interventions. Combining the two technologies is, to my mind, a natural and inevitable progression that is happening at the current time. To this end I created www.neuroinnovations.com, a software development company that is devoted to the production of software for psychotherapists of all types.
I am both a psychotherapist and a technologist. I firmly believe in the power of technology and the power of many psychotherapeutic interventions. Combining the two technologies is, to my mind, a natural and inevitable progression that is happening at the current time. To this end I created www.neuroinnovations.com, a software development company that is devoted to the production of software for psychotherapists of all types.
Many others also feel the same way and I give thanks to those that have tried and tested hundreds of ideas over the years. I also thank the novelists, science finction writers and conspiracy theroists that have primed society for what is to come and generated such a vast range of ideas for techologists to consider.
Some of those ideas may evolve into primary mainstream methodologies for the semi automated treatment of psychological disorders and for self application by the general public. The human angle will always remain but what will change (in fact what is changing) is the range of technological tools that therapists may call upon during the course of treatment and the range of self help products available to us all.
Also, just to demonstrate my support for internet technologies this "paper" has been written entirely within the internet using internet based technologies. Additionally, the table of contents, index of diagrams, listing of tables and all of the references within this paper are dynamically generated programatically as this document loads into memory.
Delimitations of scope and key assumptions
Delimitations of scope
This paper will restrict itself to technologies that directly contribute to the therapeutic process. Ancillary technologies that that are simply used by therapists for practice administration eg eMail or mobile phones is beyond the scope of this paper unless that use is very novel or substantially enhancing.
On this basis all of the following have been excluded:
- Video teleconferencing to provide therapy via video link
- eMail or messaging based provision of therapy
- Simple audio recordings
- Simple display of information on a website
- Simple swirling images that can generate trance like states
- Psychometric testing and screening eg www.psychscreen.com
This excludes philosophical self-help interventions, psycho pharmacological medications and all other chemical methods of altering mind states.
All technologies researched must be directly therapeutic in their own right or must significantly enhance or add to the therapeutic process itself.
All technologies investigated must currently exist in one form or another. This excludes conceptual ideas but includes active research.
Throughout this paper the current time shall refer to the close of 2007.
Up and coming technological solutions will be considered briefly at the close of each section.
Assumptions
It is assumed that "available" technologies have some form of presence within the internet. It is therefore possible that a technological form may exist that has not been identified because it is not present or easily identifiable through web based research. This will probably or certainly include some technologies in the domain of the Government or Military that are not in the public domain.
It is also assumed that identifiable research material will be in the English language. Hence it is possible that major blocks of research may have been missed because they were in a language other than English. This was unavoidable but justifiable on the basis that this paper is primarily concernced with technologies that are available to the general public and / or therapists throughout the world.
Defining Technology - a brief history
How we define "technology" varies over time. In Neolithic times flint tools would have been defined as "technology". A lightning tour through this technological evolution might include the following landmarks for the technology we know as "psychotherapy":
- 100,000 BC Religion / Shamanism / Mind altering drugs thought to be in use [Ref]
- 10,000 BC Alcohol first known to be used (probably earlier in fact) [Ref]
- 1700's Psychotherapy begins to evolve [Ref] [Ref]
- 1800's Self-help publications start to become popular [Ref]
- 1940's Electroconvulsive therapy (ECT) first used [Ref]
- 1950's Psychopharmacology matures [Ref]
- 1950's MK Ultra project (A purported series of experiments by the CIA to control minds) [Ref]
- 1960's Biofeedback begins to evolve [Ref]
- 1970's Computers begin to be used by therapists [Ref]
- 1980's The Internet matures into an effective method of communication and becomes more interactive [Ref]
- 1990's Computer multi-media matures [Ref] [Ref]
Arguably the most important innovations that have had the potential to affect the greatest number of people have been internet and computer related.
The internet has meant ease of access to information and easy, low cost dissemination of that information. Whilst initially the internet communicated textual information in a very static manner the evolution of web page coding languages such as JavaScript enabled web pages to become much more dynamic and interactive. [Ref]
Perhaps the most significant computer hardware related innovation has been the maturation of multi-media technologies. The meteoric evolution of multi media was in no small way driven by the demands of the computer gaming, simulation and animation markets which evolved as computers evolved. [Ref].
The net effect has been that modern personal computers can be powerful vehicles for presenting and manipulating images and sounds, as well as processing textual logic. More than any other factor this single attribute of modern computing has greatly extended the range of uses for home computers. This now substantially encompasses computer assisted psychotherapy both as an aid for therapists and for use by a therapist's patients with or without supervision from a therapist.
Media representation of psychological therapies and technologies
If media representations and myths are predictors or influencers of that which is to follow it is useful to be aware of what has been portrayed thus far:
One of the first intimated instances of mind controlling technologies in action was inferred in George Orwell's novel Nineteen Eighty Four. Although the precise details of what occurred in "Room 101" were never fully disclosed it is commonly thought to have represented a form of torture whereby the citizen would be exposed to their worst nightmares and fears as a consequence of rebelling against "Big Brother". [Ref] [Ref]
This form of "torture" can be viewed as a form of operant conditioning whereby unwanted behaviour is punished and wanted behaviour is rewarded. In the case of "Nineteen Eighty Four" the reward was being permitted to exist. [Ref]
") One of the most well known instances of technology being used to directly control thoughts and behaviours was the anti violence treatment portrayed by "A Clockwork Orange" (1971) / Anothony Burgess. [Ref] [Ref]
One of the most well known instances of technology being used to directly control thoughts and behaviours was the anti violence treatment portrayed by "A Clockwork Orange" (1971) / Anothony Burgess. [Ref] [Ref]
The fictitious events portrayed by The Clockwork Orange were replicated by the Department of Psychology, Iowa State University, USA when examining the desensitisation effect of playing violent computer games. Their conclusions indicated that there was a demonstrable physiological desensitization to violence. [Ref]
In this film the lead character was subjected to a psychological conditioning technique referred to as the "Ludovico technique" which involved forced aversion using classical conditioning. The aversion therapy took the form of being forced to see violent images whilst at the same time being exposed to a drug induced near death experience in order to remove violent behaviours. [Ref]
In the movie "The Bourne Identity (1980)" a variety of approaches were used to suppress the identity of assassin Jason Borne. These were revealed in later sequels (2004 / 2007) to have included drug based interventions combined with conditioning and behaviour modification techniques. [Ref]
In the 1996 film "Shine" portraying the life of pianist David Helfgott Electroconvulsive Therapy (ECT) was used as part of a treatment for a mental breakdown. The inference was perhaps that ECT and / or high doses of medications resulted in permanent neurological damage. [Ref]
 In the 1997 film "As Good as It Gets" Jack Nicholson portrayed a patient undergoing cognitive and drug based treatments to resolve obsessive compulsive disorder. In this instance the treatments were portrayed neutrally and in the final scenes the lead character revealed that he would finally start taking his medications as advised. [Ref]
In the 1997 film "As Good as It Gets" Jack Nicholson portrayed a patient undergoing cognitive and drug based treatments to resolve obsessive compulsive disorder. In this instance the treatments were portrayed neutrally and in the final scenes the lead character revealed that he would finally start taking his medications as advised. [Ref]
The entire genre of science fiction calls upon mind control to enliven scripts. One example might be Robert Heinlein's 1951 novel "The Puppet Masters" in which alien parasites controlled human minds. [Ref]. In the Stargate SG1 series based on the 1994 film "Stargate" in which the parasites known as the Goauld controlled their human hosts. [Ref] [Ref]
In Derren Brown's "Mind Control" series viewers were astonished by Brown's apparent ability to control how others thought and behaved. The show relied upon the power of suggestion, mental tricks, enhanced observation skills and careful post-production editing to generate the effects portrayed. [Ref]
To date media representations of psychiatric and psychotherapeutic treatments have tended to be somewhat apocalyptic because this is what tends to sell films and books. As time passes the depiction of psychological therapies appears to have become slightly more balanced and a little less prone to sensationalism. [Ref]
It is certainly true that most media depictions that portray "mind control" techniques did not represent what was currently actually possible in the real world, at that time. In the real world, in order to change how we think, feel or behave (in the main) requires the active participation and agreement of the patient. In the future this requirement may diminish.
It is perhaps also true to say that there is a general perception that technology should be able to easily facilitate "mind control" as a result of media representations. This expectation of successful outcomes also applied to more traditional forms of psychotherapy and medicine generally, both of which are of course also forms of technology.
Practical applications
Thus far we have seen how the definition of what technology is shifts over time and how there can be expectation that modern technology should be able to change how we think, feel and behave. The following sections will examine how current technologies as of 2007 are increasingly being used in the personal change process.
Hypnotherapy
Hypnotherapy can be defined as the utilisation of hypnotic states of relaxation in order to change ways of thinking and or behaving. There is considerable utilisation within the field of hypnotherapy of other psychotherapeutic approaches including NLP, CBT and EMDR. It is proposed that when these other approaches are applied when in a relaxed hypnotic state beneficial results can be maximised. [Ref]
Despite the highly auditory nature of hypnotherapy innovative ways of delivering that audio have emerged. In the first instance hypnotherapy audio was combined with relaxing video imagery and special effects were applied to certain aspects of the hypnotherapy audio. These included subliminal auditory and visual suggestions (despite the lack of supporting evidence), panning, echo, layering and resonance sound effects.
Computer and technology based approaches include:
- Generation of custom hypnotherapy downloads online
- Stand alone applications some of which allow the user to "mix and match" positive suggestions
- Hypnotherapy combined with low frequency audio
- Electronic equipment to add special effects during "live" hypnotherapy sessions
These options are discussed in more detail below.
Generation of custom hypnotherapy downloads online
A hypnotherapy session consists of four separate phases:
- Induction in order to generate initial relaxation and to obtain early eye closure
- Deepening to generate a deeper sense of physical and psychological relaxation
- Therapy to generate changes in conscious and unconscious thought patterns and behaviours
- Awakening in order to return bodily sensations to normal, to re-associate the patient and to generate an alert state of mind with the eyes open
Although the selection of an induction and deepener is often influenced by the nature of the issue, it is possible to provide generic versions of both that could apply to any condition. When this is done it is possible to enable an online web user to select their own induction, deepener and therapy of choice, and for the remote web server to generate a partially customised user defined hypnotherapy session. To further customise the process pre-recorded or computer generated patient names for example could be merged into the session.
 The "Online session builder" from www.changingstates.co.uk allows the user to construct their own session using large blocks of pre-recorded hypnosis audio. These include an induction, a deepener, some form of therapy and a standard awakening. The audio components are human generated and further customisation is not possible. [Ref]
The "Online session builder" from www.changingstates.co.uk allows the user to construct their own session using large blocks of pre-recorded hypnosis audio. These include an induction, a deepener, some form of therapy and a standard awakening. The audio components are human generated and further customisation is not possible. [Ref]
Stand alone applications
Stand alone applications such as the can also allow the user to generate their own audio either by choosing large or small blocks of suggestions that are then sequenced together by the application in real time. The major advantage of the stand-alone route is that the audio quality can be excellent because download speeds are not imposing technical restrictions.
 The "Hypno Doctor" subliminal textual messaging product from www.hypno-doctor.com primarily displays subliminal text messages to the user and therefore does not use hypnotherapy as such. In fact hypnosis would be disadvantageous given that it more or less requires eye closure that would prevent the user from seeing (or not seeing) the subliminal messages on their screen. [Ref]
The "Hypno Doctor" subliminal textual messaging product from www.hypno-doctor.com primarily displays subliminal text messages to the user and therefore does not use hypnotherapy as such. In fact hypnosis would be disadvantageous given that it more or less requires eye closure that would prevent the user from seeing (or not seeing) the subliminal messages on their screen. [Ref]
There is little or no evidence to support the contention that subliminal messages have any effect at all. None the less there is a view that they are effective and for those that strongly support that view this approach may be effective. In the UK subliminal messaging is theoretically banned from all TV programs. [Ref]
 Some products such as the offering from www.computerhometherapy.com are unusual if nothing else. In this case the therapist uses what he describes as relaxation therapy to deliver suggestions seeking to generate change. He also makes use of semi subliminal textual messaging. (Semi subliminal because the text remains on-screen for more than 1/3000 of a second). [Ref]
Some products such as the offering from www.computerhometherapy.com are unusual if nothing else. In this case the therapist uses what he describes as relaxation therapy to deliver suggestions seeking to generate change. He also makes use of semi subliminal textual messaging. (Semi subliminal because the text remains on-screen for more than 1/3000 of a second). [Ref]
Because the application is stand alone the audio quality is technically good and the series of applications from this therapist serve to illustrate a relatively simple yet effective method of playing sounds and showing images. [Ref]
 The "Virtual Hypnotist" from vhypno.sourceforge.net is a freeware software product designed as a self-hypnosis tool. Trance like states are generated through the use of flashing and swirling patterns. Suggested are provided in the form on on-screen textual messages and text to speech computer generated audio.
The "Virtual Hypnotist" from vhypno.sourceforge.net is a freeware software product designed as a self-hypnosis tool. Trance like states are generated through the use of flashing and swirling patterns. Suggested are provided in the form on on-screen textual messages and text to speech computer generated audio.
Hypnotherapy combined with low frequency audio
Hypnotherapy in particular can be combined effectively and easily with low frequency audio therapy, binaural beats and brainwave entrainment. [Ref] [Ref]
The three terms "low frequency audio therapy", "binaural beats" and "brainwave entrainment" have the following meanings (covered in more detail in the "low frequency audio" section:
Low frequency audio therapy
The use of low frequency audio stimulation to generate psychological change. With most "home" equipment this is only possible via "Binaural beats". Different frequencies generate different effects from alertness though to deep relaxation.
Binaural beats
Binaural beats generate the same effect as low frequency audio but without needing specialised audio equipment.
Brainwave entrainment
Brainwave entrainment gradually reduces the frequency of binaural beats from alertness through to deep relaxation and back to normal alertness again, or remaining in deep relaxation if sleep is the goal.
 "Hypno Studio" from www.hypnostudio.com is a stand alone application that combines text to speech computer generated vocal audio with low frequency "Binaural Beats", (bilateral stimulation) and relaxation sound effects. [Ref]
"Hypno Studio" from www.hypnostudio.com is a stand alone application that combines text to speech computer generated vocal audio with low frequency "Binaural Beats", (bilateral stimulation) and relaxation sound effects. [Ref]
Professional hypnotherapists can use the system to generate low frequency audio that can be used as a backing track for their own hypnotherapy audio CDs. Neuro Programmer provides an effective method of combining external hypnotherapy audio with low frequency audio. [Ref] (Also see Hypno Studio").
Electronic special effect equipment
Electronic special effect equipment is primarily designed for use by hypnotherapists and those involved with guided meditation. This type of equipment can be used on a one to one basis, and con sometimes be used when working with groups.
The result is a bulky package which may be of benefit to hypnotherapists that wish to apply special effects to their voices, but that do not have the basic computer literacy skills required in order to use their computer to achieve the same objective.
The computer based route is far cheaper because there is no additional investment in equipment. There can however be audio quality advantages to not being connected to a computer when making audio recordings for those affected by "electronic noise" issues. Noise removal can however be achieved less expensively by simply purchasing a Dat recorder and transferring the file to a computer, or by removing the source of the noise at source (eg switch off fluorescent lights). [Ref] [Ref]
The Future
The most promising area for future development probably lies in products that can generate hypnotherapy sessions "on the fly" by converting text into speech. This affords an almost unlimited level of customisation. However, current text to speech technologies are generally quite crude and generate audio that is very clearly commuter generated. This is in part because the computer does not "understand" what is being said therefore cannot fully adapt intonation to match what is being said. Developments in this field are highly probable and it is likely that speech generators will eventually be able to produce highly realistic computer generated speech.
Computer based hypnotherapy usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
Flooding exposure therapy
See also: Virtual reality exposure therapy
Flooding is a behavioural therapy technique in which a patient is flooded or intensely exposed with a specific experience until they either become averse or numbed to that experience. The experience may be doing or not doing a specific behaviour, or direct exposure to something that is feared in the case of phobias or that which is overly desired in the case of compulsions eg smoking. Flooding can also be applied to specific aspects of traumatic memories. [Ref]
In all cases exposure is maintained at an intense level in the absence of relaxation until the level of anxiety or desire naturally reduces. Flooding is an example of Classical Conditioning and can be conducted in vivo or in vitro (in reality / in the real world or in the imagination). [Ref]
In many cases in vivo (real world) implementation of flooding is impractical or simply unsafe. This could for example be the case for example when treating a medically discharged soldier for battle fatigue / PTSD, or when working with those that self-harm. In such cases a less direct method of exposure would be strongly advantageous. One option is to expose a patient to digital or physical photographic images in an intense manner. [Ref] [Ref]
 "Flooder" from www.neuroinnovations.com is designed to automate the flooding process by allowing the user to select one or more images that are zoomed onto or off the screen rapidly. At the same time user selected audio is played with the option to pulse the volume in sync with the image movements. The user controls the speed of image presentation and can stop all movement and sound instantly.
"Flooder" from www.neuroinnovations.com is designed to automate the flooding process by allowing the user to select one or more images that are zoomed onto or off the screen rapidly. At the same time user selected audio is played with the option to pulse the volume in sync with the image movements. The user controls the speed of image presentation and can stop all movement and sound instantly.
The probable application of this form of computer based flooding / implosion therapy include desensitisation of memories, installation of aversion, reducing food, alcohol and drug based compulsions, reducing fears related to specific objects or animals, reducing the blush response in cases where excessive blushing has become associated with specific words or images. The approach lies somewhere between in vivo and in vitro styles.
Flooding is however not without risk - there is a danger of (re)traumatisation. The most common problem is that therapists or patients discontinue the approach before the level of anxiety or desire has had an opportunity to naturally reduce or abate. This early termination can leave the patient in a sensitised state of hyper arousal that may complicate later therapeutic interventions or lead to the premature termination of therapy altogether. For this reason informed patient consent is vitally important to ensure that the process is allowed to complete. Even with informed patient consent there is no absolute guarantee that the level of disturbance or desire will diminish. Hence, particularly when working with traumatic memories or fears, flooding should be employed carefully. In most cases flooding should be used as an intervention of last resort having tried other approaches without success first.
An exception to this general rule might be where aversion is the goal of the process, in which case the end result may justify the means in order to limit further harm. Aversion through flooding or by any other means should be considered from an ethical perspective whereby the therapist may need to balance the potential damage that may result from the continuance of the behaviour versus the potential risks due to the therapeutic process itself.
A more common place role for flooding is as a training and conditioning tool. This form of flooding is part of military, special forces, police, police armed unit, air pilot, air crew and fire / ambulance training programmes. In most cases in vivo experiences are simulated to ensure that trainees can cope effectively in high stress or otherwise distressing situations. In the case of pilot training and ongoing evaluation computer based simulations have become the "norm" in many parts of the world. [Ref] [Ref]
Flooding usage summary:
|
To install aversive responses:
|
De-traumatisation
|
De-sensitisation
|
Methods
|
In cases where the danger of retraumatisation is too great a gentler, more gradual approach to exposure therapy tends to be adopted. The title for this broad category of approaches is often referred to as "systemic desensitisation".
See also systemic desensitisation.
Virtual Reality Exposure Therapy
 In vivo flying desensitisation through the use of virtual reality environments has also seen some success, but is slightly more limited given the high cost of the specialised equipment. [Ref]. Virtual reality flooding (exposure therapy) approaches have also been used in the treatment of combat related PTSD (Post Traumatic Stress Disorder). Veterans from the Vietnam [Ref] and Iraq conflicts [Ref] have taken part in promising early trials. [Ref]
In vivo flying desensitisation through the use of virtual reality environments has also seen some success, but is slightly more limited given the high cost of the specialised equipment. [Ref]. Virtual reality flooding (exposure therapy) approaches have also been used in the treatment of combat related PTSD (Post Traumatic Stress Disorder). Veterans from the Vietnam [Ref] and Iraq conflicts [Ref] have taken part in promising early trials. [Ref]
Simpler alternatives to virtual reality are clearly viable. For example therapists could make use of multi media presentations that combine static images or videos and related sounds in such a way that combat scenarios can be emulated. This approach would not require investment in virtual reality systems and would therefore be easier to implement en-mass. Washington University treated 9/11 survivors with virtual reality simulations and also released video footage for therapists without access to the University's extensive virtual reality resources and systems. [Ref]
One of the earliest therapeutic uses of virtual reality was in the treatment of phobias including flying, spider and height phobias. Exposure can be gradual enabling systemic or gradual desensitisation, or could feasibly be used to implement flooding approaches. [Ref]
Multimedia compilations are also available to assist in the treatment of combat / war related trauma. The combat experience is simulated by providing a number of graded categories of media to choose from in order to gradually desensitise to traumatic stimuli. Such media can be utilised within flooding or systemic desensitisation approaches. [Ref]
Virtual reality has also been used in the treatment of agoraphobia (fear of being in open spaces / fear of loss of control in open spaces (public) / fear of having a panic attack in public) [Ref] [Ref] and public transport phobias. [Ref]
 "NeuroVR" is a freeware virtual reality product from www.neurovr.org. The system can work with specialist VR headsets and is pre-supplied with a variety of virtual reality scenes including a supermarket, elevator, office and restaurant. Image quality is reasonable given that the system is open-source freeware. The scenes packaged with the product are suitable for use when treating panic disorder patients.
"NeuroVR" is a freeware virtual reality product from www.neurovr.org. The system can work with specialist VR headsets and is pre-supplied with a variety of virtual reality scenes including a supermarket, elevator, office and restaurant. Image quality is reasonable given that the system is open-source freeware. The scenes packaged with the product are suitable for use when treating panic disorder patients.
Virtual Reality Exposure Therapy usage summary:
|
To treat phobias and fears:
|
De-traumatisation
|
De-sensitisation
|
Methods
|
Systematic gradual desensitisation exposure therapy
See also: Virtual reality exposure therapy / Flooding / EMDR / Computer-assisted exposure (CAE) treatment
Systemic gradual desensitisation exposure therapy, or systemic desensitisation, is a behavioural therapy that involves modifying behaviours by constructing a hierarchy of anxiety producing stimuli and then gradually presenting them to a patient until they do not generate anxiety. During the process the therapist actively supports the patient and encourages relaxation. The reverse approach tends to be adopted in the case of traditional flooding desensitisation whereby the stress response is allowed to extinguish itself naturally. [Ref] [Ref]
The hierarchy is known variously as the Subjective Units of Disturbance / Distress / Urge Scale (SUDS) and tends to be numerical eg 0 to 10, or 1 to 100; or sometimes visual as is the case with the Wong Baker scale for children when adapted for use with anxiety / distress. [Ref] [Ref] Numerical responses lend themselves well to computerisation and can be used to enable effective user interaction during the therapeutic process.
Technologies used for flooding can be easily utilised for systematic desensitisation therapy simply by flooding gradually in accordance with a hierarchy as per systematic desensitisation. [Ref] This approach is also sometimes known as graded exposure. [Ref]
The stimuli may be presented in the imagination (in vitro) or in the real world (in vivo). Early in vivo use of technology to assist with systematic desensitisation therapy included the use of graded photographic images, videos and drawings. [Ref]
Early web technology based approaches simply grouped image and audio stimuli into categories which would then be presented to the user. The disadvantage of this approach is that stimuli hierarchies are highly individual and media that would be low on one person's hierarchy might be high on another person's hierarchy. [Ref]
Computer assisted approaches evolved over time as multi media computer technologies matured. One method was to use a multimedia computer to gradually present a user selected image that was initially so small that it was almost invisible. Over time the image is made larger as the level of anxiety produced decreased. [Ref]
 Vivo" from www.neuroinnovations.com allows the user to select a single image and to gradually increase the size of the image from a tiny dot to full-screen.
Vivo" from www.neuroinnovations.com allows the user to select a single image and to gradually increase the size of the image from a tiny dot to full-screen.
Vivo is a freeware product and is also part of the product "Flooder" detailed above. The ability to play audio from within the product is not present in Vivo, but is present in Flooder.
More advanced implementations used the processing power of computers to enable interaction and dialogue. Methods of distributing such media included via the Internet, CD-ROMs and interactive DVDs. [Ref] [Ref] [Ref]
Some NLP Techniques such as the Map Across or Swish techniques utilise interactive computer animations to generate computer based utilities that can be used as part of a systemic desensitisation programme. In cases where the imagery is defined by the user or therapist this type of approach may be particularly effective by combining several psychotherapeutic techniques into one overall approach. [Ref] [Ref] [Ref] [Ref]
Self help DVD's were available that in effect used the DVD format as an alternative to video ie with little or no user interaction. (DVDs allow interaction by allowing the user to navigate in a structured manner through a network of interrelated video clips). [Ref]
Virtual reality exposure therapy can enable moderately to highly realistic stimuli exposure, potentially with the user being able to control the extent of exposure. From the perspective of systematic desensitisation therapy this realism can be both an advantage as well as a disadvantage depending on how gradual the stimuli presentation is. Virtual reality systems tend to have preset scenes through which the user navigates. As with all forms of media presentation if the scenes do not cover the entire range of possible categories on the SUDS scale then the approach may be limited and / or insufficiently flexible. If the scenes are too realistic and presented too early there is the same danger of (re)traumatisation that is present with flooding. [Ref] [Ref]
The conclusion of all forms of exposure therapy should be literal in vivo (in reality) exposure, unless that exposure might result in physical harm eg as might be the case with a (legitimate) fear of poisonous snakes. In most cases in vitro (in the imagination) exposure should be working towards this goal to overcome the avoidance that maintains the phobic response. In the case of flying phobia this might involve taking a specially organised flight. [Ref]
EMDR (Eye Movement Desensitisation and Reprocessing) can be used as a systemic desensitisation tool depending on the protocols being used. (See EMDR section for further information).
Systematic desensitisation usage summary:
|
To treat phobias and fears:
|
De-traumatisation
|
De-sensitisation
|
Methods
|
CBT - Cognitive Behavioural Therapy / Cognitive Behaviour Hypnotherapy
Cognitive Behavioural Therapy (CBT) is a psychotherapeutic approach that involves the modification of cognitions (thoughts), assumptions, beliefs and behaviours in order to resolve emotional and behavioural problems. These include depression and a wide range of anxiety based issues such as OCDs. CBT evolved from Behavioural Therapy, Cognitive Therapy and Rational Emotive Behaviour Therapy and is probably the most common "mainstream" therapeutic approach in use today.
Techniques used within CBT are numerous and include diary keeping, scaling feelings over time, writing thoughts down, documenting behaviours, tasking generally, relaxation, distraction, questioning ways of thinking, evaluating and believing, reversing avoidance gradually and changing behaviours with or without changing underlying thinking patterns. CBT can used on a one to one basis, or with groups. [Ref]
CBT is very well suited to computerisation because it is so textual and logical. As a result CBT has influenced many self help resources including books, DVDs, interactive websites and software systems.
The logical flow within a CBT application might look something like the following:
- Are you depressed or anxious?
- If depressed:
- Provide anxiety related advice
- Teach the user a positive thinking technique
- Go back to start
- If anxious:
- Provide depression related advice
- Teach the user a relaxation technique
- Go back to start
- If depressed:
Quite complex logical can be built up by expanding upon this very simple logical format. The more advanced the interaction becomes the more personalised the experience will be for the end user. In an advanced application the user might be asked to complete questionnaires that are evaluated programmatically to determine if the person is more anxious or depressed.
A few the software and web based resources currently available include "MoodGYM", "Beating the Blues", "Good Days Ahead", "COPE" and "Overcoming" for the treatment of mild and moderate depression, and "FearFighter" or "OCFighter" for the treatment of phobias and OCDs, and "The Stress and Anxiety Manager" for the treatment of stress and anxiety. Some, but not all, have NICE approval (National Institute for Health and Clinical Excellence). [Ref]
 "The Stress and Anxiety Manager" from Changing States is an online approach to the treatment of stress of and anxiety that uses a combination of:
"The Stress and Anxiety Manager" from Changing States is an online approach to the treatment of stress of and anxiety that uses a combination of:
- CBT
- hypnotherapy
- online EMDR
- low frequency audio
The programme is part of a clinical trial and before and after data is collected. Treatment is provided via animated speaking Flash characters, Flash animations to support the dialogue, downloadable audio files and online EMDR.
https://www.changingstates.co.uk/stress_anxiety_treatment_online.html [Ref]
 "MoodGYM" is free to access, interactive website built using Flash and Asp. The site is hosted on Australian servers and does contain some terms that may be more suited to an Australian audience eg "unwarping". [Ref] [Ref]
"MoodGYM" is free to access, interactive website built using Flash and Asp. The site is hosted on Australian servers and does contain some terms that may be more suited to an Australian audience eg "unwarping". [Ref] [Ref]
The site uses a series of questionnaires or quizzes with contextually appropriate advice at regular intervals based on quiz results and self comparison to positive and negative archetypal or stereotypical personality types. The character "NOPROBLEMOS" for example is described as "one of those people who are genuinely happy, self fulfilled, loves life, is content".
The quizzes are split into a number of modules including 'preliminary quizzes', 'feelings module', 'thoughts module', 'unwarping module', 'de-stressing module', 'relationships module' which seek to target different aspects of anxiety and depression.
 According to those that market "Beating the Blues" is the UK market leader in online CBT solutions and certainly has broad uptake within the NHS. "Beating the Blues" had NICE approved at the time of writing hence the strong uptake within the NHS.
According to those that market "Beating the Blues" is the UK market leader in online CBT solutions and certainly has broad uptake within the NHS. "Beating the Blues" had NICE approved at the time of writing hence the strong uptake within the NHS.
Access to the resource is not free as such given that referral must be via a patient's GP or mental health worker. The area's Primary Care Trust then pays for that patient's access to the beatingtheblues.co.uk website via an activation code. [Ref] [Ref]
 "Beating the Blues" makes use of interactive Flash animations with voice-overs and includes filmed case studies of actors playing the roles of fictional patients to demonstrate the symptoms of anxiety and depression.
"Beating the Blues" makes use of interactive Flash animations with voice-overs and includes filmed case studies of actors playing the roles of fictional patients to demonstrate the symptoms of anxiety and depression.
The actors also show how to use self-help CBT techniques such as relaxation via controlled breathing (see screenshot to right). Over the course of the eight session treatment patients are able to print off summary progress reports to show to their GPs. [Ref]
A major disadvantage of interactive websites that feature video feeds as a substantial part of the service offering is that this almost requires good quality broadband access to the internet. If the speed of internet access is insufficient user may experience long pauses, video juddering or skipping and sometimes system failure.
The unavailability of web based resources as demonstrated by the "Overcoming depression" website does reveal some of the pitfalls of web based media. The most important of which is that the resource may not be available when a patient needs it most. Other issues include technical compatibility from the outset and compatibility over time given that browsers can update themselves without user intervention.
Although DVDs do eliminate the need for high speed, reliable internet connections they tend to have greatly reduced interactive abilities. DVDs are also prone to scratch damage that may render the DVD unusable. The video quality afforded by the DVD format is however excellent.
The patient identifies problems to work through, defines outcome goals and is guided through the process of attaining those goals through a process of gradual exposure self therapy. [Ref]
As is the case with all therapies there is a risk that the patient will discontinue therapy before the conclusion of the programme. Whilst this can also be the case with one to one therapy the risk is probably increased without the ongoing supervision that is present within the nature of one to one therapeutic relationships. Solutions that require GP involvement may provide this external encouragement if the GP has the time and willingness to monitor ongoing progress.
To summarise there are broadly three categories of interactive CBT self-help support available:
- Telephone based
- DVD based
- Web based
All of the categories are interactive to a greater or lesser extent and provide supporting reading material as part of the service. It is interesting to note that, in the UK at least, access to the resources often requires GP approval. It may be the case that this elevates the value that patients attribute to the service ie restricting supply to increase demand.
Other resources:
Some products are designed for use by therapists rather than for use by patients. These include practice management and patient communication software products. Practice management software products include features such as billing, standard letter production and session records. Patient communication products handle appointment scheduling and reminding. One example is Practice Magic from Cornucopia Software. These administrative programs are beyond the scope of this paper because they are not directly involved in the provision of therapy. [Ref]
One of the most common tasks that CBT therapists engage in is tasking itself - at the end of most sessions the therapist gives the patient a list of things to do. This process is known as tasking.
 "Tasker" from www.neuroinnovations.com automates tasking by providing the therapist with a list of common tasks to select from that can then be sent by eMail to their patient. The therapist has the ability to customise the eMail subject field, the option to print the task list rather than sending it by eMail and the ability to edit the task list at will, and include non standard ad hoc tasks. [Ref]
"Tasker" from www.neuroinnovations.com automates tasking by providing the therapist with a list of common tasks to select from that can then be sent by eMail to their patient. The therapist has the ability to customise the eMail subject field, the option to print the task list rather than sending it by eMail and the ability to edit the task list at will, and include non standard ad hoc tasks. [Ref]
Although tasking can be automated the disadvantage of this approach is that it has the potential to reduce the level of personal intervention on the part of the therapist. This could be construed by the patient as a lack of due care and attention to their needs and wants. Also, some therapists deliberately want their patients to take responsibility for the generation of their own task list. For some patients with poor memory retention as might be the case with anxiety or depression it may be impractical to expect them to exactly remember tasks communicated verbally during the therapy session.
Computer based Cognitive Behavioural Therapy (CBT) usage summary:
|
To treat:
|
Techniques / style:
|
Methods
|
Counselling
Counselling can be defined as a confidential, short-term, semi-therapeutic interpersonal relationship to help those that are essentially psychologically healthy through emotionally challenging times. [Ref] [Ref] [Ref] [Ref]
There are a wide variety of counselling approaches that are more or less therapeutic in nature. Psychodynamic counselling for example is highly directive and based on the theory that issues are rooted in the past, whereas more humanistic Rogerian approaches are highly un-directive and are very much more driven by the individual needs of the patient. [Ref]
Common aspects of counselling include an interpersonal relationship and dialogue that allows the patient to express themselves openly and confidentially. Online counselling has been available for some time and simply involves a counsellor using eMail and or the telephone as an alternative to face to face counselling. [Ref]
Traditional uses of technology within counselling include the use of DVDs, simple informational websites, websites that contain informational video content eg www.kpcoach.org [Ref].
Beyond this, forms of counselling that employ technology without the direct presence of a human therapist are much less common than human based approaches but do exist.
A very early form of computer based counselling was in the form of Eliza. Eliza was a computer program developed in the late 60s that provided a "parody" of "the responses of a non-directional psychotherapist in an initial psychiatric interview." It used simple programming techniques to incorporate user responses into questions eg "I have a headache" would result in "Tell me more about your headache" or "Can you elaborate on that?" if the word headache was not understood. Users were however able to detect that there was little or no "thought" behind the process very quickly. Click here to experience a simulation of the Eliza effect. [Ref] [Ref]
 In the real world the simplest form of interactive virtual counselling can simply involve asking questions via a web-form and providing different advice depending on the responses provided. The advice can sometimes incorporate the responses given by the user eg their name. Some websites for example provide this type of service eg in relation to alcohol consumption. [Ref]
In the real world the simplest form of interactive virtual counselling can simply involve asking questions via a web-form and providing different advice depending on the responses provided. The advice can sometimes incorporate the responses given by the user eg their name. Some websites for example provide this type of service eg in relation to alcohol consumption. [Ref]
 This method of providing interaction can be extended to telephone based services and can be used as part of stand alone applications. One historical example is an early product known as UCANSTOP that was designed as an alcohol counselling resource. A current provider of the product mentioned could not be found at the time of writing.
This method of providing interaction can be extended to telephone based services and can be used as part of stand alone applications. One historical example is an early product known as UCANSTOP that was designed as an alcohol counselling resource. A current provider of the product mentioned could not be found at the time of writing.
Research into the field of truly virtual counselling has been ongoing for many years. In the 1980s for example the Dilemma counselling system "Dilemma counselling system" was proposed. More recently there has been research conducted by the University of Dundee on the use of computers to make computer based interviewing more effective and realistically interactive. It was unclear at the time of writing if this research had evolved into a viable current product. [Ref] [Ref] [Ref]
Advances in natural language processing, artificial intelligence and expert systems since the 1990s have held much promise but there are very few easily identifiable examples of such systems being actively used in the provision of virtual counselling services. [Ref]
A potentially promising collaboration between British Telecom and onlinecounsellors.co.uk resulted in what may have been a viable counselling related use of avatars, but the service had been discontinued at the time of writing. [Ref]
Recent innovations in emotion detection have enabled call centres to detect frustration or annoyance through the analysis of customers' speech patterns. Although still very costly it is likely that this technology could be adapted for use by computer based "counsellors" to detect change over time during the course of the session in order to display an appropriate facial expression for example. [Ref]
The Future
In the future it is probable that improvements in language processing, voice recognition, artificial intelligence and distributed knowledge bases will make the automated dissemination of advice and realistic counselling interactions more economically feasible. This form of "front line" initial response could serve as an effective precursor to one to one therapy with a human therapist. The combined technology is present at the current time but demand may be insufficient to warrant the substantial investment required to build the required knowledge databases.
It is probable that computer based expert systems can be developed to make use of NLP meta modelling style questioning techniques. Such systems could deconstruct a patient's conversational patterns and respond with standard meta model questions that are designed to generate insight. An early experimental form of this approach was developed by www.neuroinnovations.com [Ref] [Ref]
One factor that is highly likely to inhibit demand is a general dislike of the "call centre" / "automated telephone system" approach to human computer interaction. If however the technology matures to the point of delivering services that deliver genuine value rather than frustration, then this generally negative perception may change.
Computer based Counselling therapy usage summary:
|
To treat:
|
Techniques / style:
|
Methods
|
Aversion Therapy
Aversion therapy can be defined as a psychotherapeutic technique in which a patient is exposed to a overly desired stimulus and at the same time also exposed to some form of discomfort. The discomfort may be physical or psychological, examples include drugs that generate nausea or a series of disgusting images. The objective of the process is to generate a conditioned response so that when the overly desired stimulus is encountered it generates a sense of aversion. In turn this can change behaviours. Aversion makes use of innate survival responses present within all animals. [Ref] [Ref]
Aversion is typically used as a technique of last resort for use when other approaches have failed to generate the desired change in behaviour. In most cases aversion requires the buy-in or active agreement of the patient. If this agreement is not present the patient may choose to ignore the resulting sense of eg disgust and proceed with the unwanted behaviour anyway. This reaction is sometimes the case with advanced substance abuse cases. Aversion is generally regarded as relatively ineffective as the sole treatment for addictions, in part this is because the aversive response is typically short-lived. [Ref] [Ref]
Another problem associated with aversion is that different people react to different stimuli in different ways. Whilst the smell of an ash tray might be a nauseous experience for one person someone else might have no reaction at all to exactly the same smell. Ironically aversion tends to be least effective with those that "need" it most, in part because they have already desensitised themselves to aversive stimuli. None the less aversion does have a role to play even if that role is simply as part of an overall range of solutions. This will certainly be case with addictions in cases where "everything" is thrown at the problem in order to improve overall success rates and to prevent further harm.
A variety of technological approaches have been used to assist in aversion therapy. In the 1970's electric shocks were experimented with but the practice is rare at the current time given the potential risks to physical health involved. Drugs that generate nausea eg in the presence of alcohol (emetics such as antabuse) are still prescribed by GPs on a regular basis. Drugs that block the effects of consumption of drugs and alcohol are available - these include Naltrexone. [Ref] [Ref] [Ref]
Some products intended for health education can be indirectly aversive. Examples might include moulded replica's of human fat, aversive images on cigarette packs, and educational videos that communicate health warnings in an aversive way. These approaches may be affective because they re-associate consequences with behaviours. [Ref] [Ref] [Ref]
Modern multimedia PC systems can provide an effective delivery method to present aversive stimuli in the forms of images and sounds. The number of products that make use of this capability is limited because the market is very small. This is in part because therapists are sometimes reluctant to use aversion as a matter of course, patients also tend to be averse to aversion because (by definition) it tends to be unpleasant.
 The "NLP Map Across - Aversion" series of software programs from www.neuroinnovations.com are designed to generate aversive responses using the NLP Map Across technique. The aversive stimuli is in the form of dog excrement combined with vomiting sounds. [Ref]
The "NLP Map Across - Aversion" series of software programs from www.neuroinnovations.com are designed to generate aversive responses using the NLP Map Across technique. The aversive stimuli is in the form of dog excrement combined with vomiting sounds. [Ref]
Aversive multimedia (generally images and sounds) can be integrated into a number of psychotherapeutic techniques including:
- Neuro Linguistic Programming (NLP) (eg the Map Across technique or anchoring)
- Eye Movement Desensitisation and Reprocessing (EMDR - see below)
- Cognitive Behavioural Therapy (Traditional aversive conditioning)
- Hypnotherapy (Aversive approaches)
- Potentially with low frequency audio (Some audio frequencies can generate nausea - but specialised equipment is generally required)
The following images are from an EMDR software product and show images of food (in these examples a chocolate cake) being associated with images of maggots or excreta).
 
|
Despite the lack of success attributed to aversive techniques aversion remains a core aspect of Government health education campaigns.
The Future
In the future it is likely that aversion will persist as a tool to call upon in cases where other treatments have been unsuccessful. A combination of drug based and therapy based aversive protocols may result in improved success rates.
Computer based Aversion Therapy usage summary:
|
To treat:
|
Techniques / style:
|
Methods
|
EMDR - Eye Movement Desensitisation and Reprocessing
Eye Movement Desensitisation and Reprocessing (EMDR) therapy can be defined as a therapeutic approach to facilitate the rapid resolution of traumas or distressing events such as assault, combat and rape. In practical terms this means that a patient is asked to think about an aspect of an experience at the same time as moving their eyes from left to right, or listening to sounds that track from left to right, or experiencing shoulder or knee taps that again track from left to right. In summary the patient thinks about something specific and experiences one or more forms of bilateral stimulation at the same time. Bilateral stimulation is anything that tracks left to right and back again. The patient is treated in accordance with a logical, step wise protocol and is asked to rank their level of disturbance on a scale at regular intervals during the process. [Ref]
The term "Eye Movement Desensitisation and Reprocessing" was first coined by Francine Shapiro in the 1990s. [Ref] The psychotherapeutic technology of using eye movements and or bilateral stimulation greatly predates Shapiro's works. These include eye movement research in the 1960s that influenced NLP eye accessing cue theories, NLP techniques such as the Swish or Map Across techniques, and hypnotherapy techniques such as systematic hypno desensitisation. Additionally substantial aspects of CBT are clearly employed during the treatment process such as distraction, systemic desensitisation, flooding desensitisation and Subjective Units of Disturbance (SUDS) ranking over time. [Ref]
It was originally proposed that the patient should track their therapists fingers, or listen to sounds generated by mechanical clicking devices operated by the therapist manually. By virtue of the close proximity of the therapist to the patient during treatments traditional methods certainly raised physical boundary issues. There are also physical dangers to the therapist that can result from the movements themselves eg repetitive strain injury.
Perhaps as a result of some of these issues a variety of technologies emerged to automate EMDR therapy. In fact so many products and technologies were produced that the market was in effect saturated. As this happened interest in EMDR as a "new" therapy naturally waned as EMDR therapy matured and lost the "novelty" factor. Those technologies included the following:
Simple audio CDs
Perhaps the first attempt to automate EMDR was when bilateral audio CDs were produced. Simple audio CDs enable very easy access to bilateral auditory stimulation via any CD player. The most obvious disadvantage is that there is limited control over the speed of the left-right tracking and there is no visual stimulation. The quality of the audio and the special effects applied to generate the bilateral effect can however be impressive and certainly very pleasant to listen to. [Ref] Other forms of bilateral audio are less technically sophisticated but none the less provide a simple and portable method of generating bilateral audio. [Ref]
Physical devices
 Probably the earliest technology to be utilised was based on large electronic devices that generated visual movement via flashing lights and auditory stimuli via external loud speakers. The sense of visual movement was generated by a long strip of light emitting diodes (LEDs) controlled by a small micro processor. This type of device is known as a light-bar.
Probably the earliest technology to be utilised was based on large electronic devices that generated visual movement via flashing lights and auditory stimuli via external loud speakers. The sense of visual movement was generated by a long strip of light emitting diodes (LEDs) controlled by a small micro processor. This type of device is known as a light-bar.
Light-bars generate movement in a straight line that can be adjusted around a central pivotal point. This generates a 360°s; possible tracking paths. The light-bar has to be moved manually by the therapist in order to change the tracking path.
Although designed to be portable these systems tended be quite heavy and cumbersome. Later versions were lighter but remained cumbersome and difficult to transport. Because of the lack of true mass production the cost tended to high as well with a typical device costing in the region of $500 USD. Many are packaged with tactile stimulators.
 Smaller electronic devices deigned to provide auditory stimulation were developed to enable greater therapist mobility. Such devices have also been used by some patients for self application of EMDR. This may be appropriate for those that are particularly sensitive to auditory stimulation.
Smaller electronic devices deigned to provide auditory stimulation were developed to enable greater therapist mobility. Such devices have also been used by some patients for self application of EMDR. This may be appropriate for those that are particularly sensitive to auditory stimulation.
As a result of the size, weight and portability issues this type of equipment has tended to be used by therapists that use EMDR very extensively within their practice as a primary intervention. Early reliability issues have largely been overcome as the electronics industry has advanced.
 Devices capable of providing tactile stimulation were developed at around the same time. Such devices would sometimes synchronise with an audio signal so that visual, auditory and tactile bilateral stimuli could be provided at the same time.
Devices capable of providing tactile stimulation were developed at around the same time. Such devices would sometimes synchronise with an audio signal so that visual, auditory and tactile bilateral stimuli could be provided at the same time.
As mobile phone "vibration sounding" motors became smaller and more powerful so the tactile tapping devices became smaller and more reliable. (The vibration is typically generated by a small motor that spins an unevenly weighted wheel).
Software
EMDR is very easily computerised and improvements in the basic specification of common PCs have greatly improved the quality of PC based animation. It is animation that generates the visual effect of an object moving across the screen. Auditory bilateral stimulation is provided via multimedia speakers or headphones, and kinaesthetic stimulation can be provided by using one of the physical tapping products listed above.
The standard features that most software based EMDR products provide are:
- Ability to select a tracking object (the image that moves from left to right)
- Ability to select a beep sound that pans from left to right in sync with the tracking object or image
- Ability to change the trajectory of the tracking object
- Ability to change the speed of the tracking object
- Ability to count the number of loops or iterations ie left to right and back again
A notable difference between software based and light-bar based EMDR systems is the extent of the left-right tracking (with the light-bar or screen at the same distance from the patient). Essentially light-bars tend to be wider than most computer screens, hence to obtain the same extent of tracking the computer screen would need to be very close to the patient. It is however not proven that the extent of tracking has a significant impact on the outcome of the therapeutic process. Some EMDR software users obviate this problem by using projectors or wide-screens.
Another difference is that software can generate tracking path changes very much more easily during the course of therapy. The tracking paths themselves can also deviate away from simple straight lines and can incorporate circular, oval and other more complex motions.
When the tracking path does not have to pass through a point of origin it is possible to track at the top, middle and bottom of the screen. As per NLP eye accessing cue theory this means that different modalities can be accessed very rapidly only by changing the tracking path. The top of the screen accesses visual thinking, the middle of the screen auditory thinking and the bottom of the screen accesses kinaesthetic thinking. This means that there is no need for tactile pulsing boxes which can be difficult to operate and utilise effectively.
 "There and Back" from www.practicemagic.com is a simple, free method of automating EMDR treatment via software. It is probably one of the first attempts to do so.
"There and Back" from www.practicemagic.com is a simple, free method of automating EMDR treatment via software. It is probably one of the first attempts to do so.
Auditory stimulation is provided via the ability to select a wave "beep" file which is played in the left or right hand speakers whenever the object tracking across the screen reaches the left or right hand sides of the screen.
Visual stimulation is provided by allowing the user to select an icon or an image file in bitmap format. If a bitmap format image file is selected the user is expected to ensure that the image is of a reasonable size. If the image is larger than about 50% of the screen width it is automatically resized so it fits on the screen.
The tracking object can move in lines using 4 preset trajectories ie up / down, left / right, top left / bottom right, bottom left / top right. Tracking speed is also adjustable.
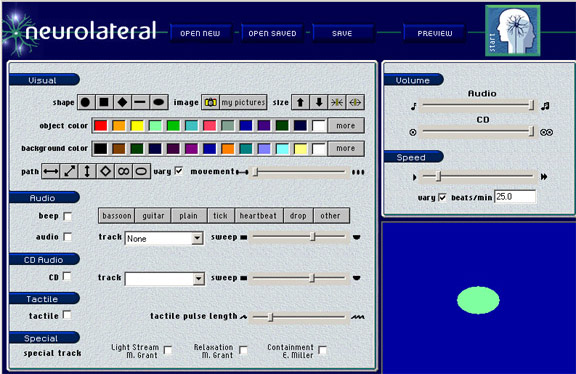 "Neuro-Láteral" is a slightly more advanced form of EMDR software with additional features including the ability to change the size of the tracking object and the ability to play background music. Background audio in the form of an audio file or a CD track can also be panned in sync with the tracking motion. It is also possible to save and load settings, to record audio output and to optionally generate variation to prevent habituation. They also market tactile units and EMDR audio CDs generated by third parties. Their tactile units only work with their EMDR software.
"Neuro-Láteral" is a slightly more advanced form of EMDR software with additional features including the ability to change the size of the tracking object and the ability to play background music. Background audio in the form of an audio file or a CD track can also be panned in sync with the tracking motion. It is also possible to save and load settings, to record audio output and to optionally generate variation to prevent habituation. They also market tactile units and EMDR audio CDs generated by third parties. Their tactile units only work with their EMDR software.
They were not contactable at the time of writing.
 "EMDR Pro" from www.neuroinnovations provides all of the standard features listed above and also provides the following:
Two layers of background audio, both of which can be panned in sync with the tracking motion; Almost unlimited tracking motions including ovals, circles, lines, elliptical lines, figure of eight, wave patterns (up and down plus right to left and back again; Ability to change the tracking direction at any time in any plane (not restricted to lines that pass though a central point on the screen); Automatic anti-habituation; Ability to play audio behind video files; Ability to play low frequency audio without distortion; Ability to display video content in the centre of the screen; Ability to make very high quality recordings via in-built sound recorder; Ability to display background images as well as background colours; Ability to change the aspect ratio of the tracking image / object; Semi subliminal display of brief textual messages to direct processing if required; Preset image shapes available in several colours or user specified images used as the tracking object; Saving / reloading of settings; Smooth starting and stopping of audio files (volume gradually increases and decreases when audio is loaded or unloaded) to avoid jarring; Includes a lite version for client use; Includes a very large user multi media library that facilitates multimedia based systemic and flooding desensitisation; Includes EMDR protocol forms and instructions; Includes multi-screen support; Very smooth animation over a wide variety of systems; Inbuilt software to demonstrate the NLP Swish technique; Also includes Tactile Units what work with or without the presence of EMDR Pro.
"EMDR Pro" from www.neuroinnovations provides all of the standard features listed above and also provides the following:
Two layers of background audio, both of which can be panned in sync with the tracking motion; Almost unlimited tracking motions including ovals, circles, lines, elliptical lines, figure of eight, wave patterns (up and down plus right to left and back again; Ability to change the tracking direction at any time in any plane (not restricted to lines that pass though a central point on the screen); Automatic anti-habituation; Ability to play audio behind video files; Ability to play low frequency audio without distortion; Ability to display video content in the centre of the screen; Ability to make very high quality recordings via in-built sound recorder; Ability to display background images as well as background colours; Ability to change the aspect ratio of the tracking image / object; Semi subliminal display of brief textual messages to direct processing if required; Preset image shapes available in several colours or user specified images used as the tracking object; Saving / reloading of settings; Smooth starting and stopping of audio files (volume gradually increases and decreases when audio is loaded or unloaded) to avoid jarring; Includes a lite version for client use; Includes a very large user multi media library that facilitates multimedia based systemic and flooding desensitisation; Includes EMDR protocol forms and instructions; Includes multi-screen support; Very smooth animation over a wide variety of systems; Inbuilt software to demonstrate the NLP Swish technique; Also includes Tactile Units what work with or without the presence of EMDR Pro.
EMDR Pro is optionally part of a much larger product known as the "Therapists Toolkit". [Ref] The "Therapists Toolkit" brings a variety of psychotherapeutic methods together into one overall product. These methods include EMDR itself, NLP, aversion, bilateral audio, EFT (the emotional freedom technique) and hypnotherapy. NLP techniques include the map across technique and the Swish technique.
Computer controlled Tactile units are available from Neuro Innovations that operate with or without the presence of EMDR Pro.
Other EMDR software products include those designed simply to generate bilateral auditory stimulation. This can be generated "on the fly" as audio is being played, or can be applied to a sound file as a "sound effect". The ability to record the audio produced can be present within the application itself or may rely upon external third party freeware solutions to achieve the same objective.
 "Bilat" from www.neuroinnovations allows the user to specify an audio source (a file or CD audio track) and a bilateral tracking speed, and then pans the audio from left to right as the audio is played. A visual indicator of the tracking speed is provided. Volume levels, pause and rewind features are also available.
"Bilat" from www.neuroinnovations allows the user to specify an audio source (a file or CD audio track) and a bilateral tracking speed, and then pans the audio from left to right as the audio is played. A visual indicator of the tracking speed is provided. Volume levels, pause and rewind features are also available.
A recording facility was not present within the product itself. However, instructions for recording the bilateral audio to file via free external software were provided on the support website.
Other similar solutions included http://www.alternant.com (download unavailable / site unavailable at the time of writing) http://www.alternant.com/5_Acquiring_the_Irenes/52%20download.asp.
The Future
The future of the EMDR technologies is somewhat dependent upon the status of EMDR and the various other eye movement based therapies. Acceptance of EMDR by therapists is limited because there is a deliberate restriction placed upon the communication of EMDR protocols. In practical terms knowledge of EMDR usage is kept in-house within a relatively small community of EMDR therapists. This tends to generate suspicion among other therapists that in turn can lead to scepticism and claims that EMDR is little more than a re-branding of well established CBT techniques.
None the less, despite the very small market, it is likely that eye movement therapy software will continue to be an important tool within a professional therapist's overall toolkit of methods. From a technical perspective it is likely that EMDR will continue to be integrated with other therapeutic methods as demonstrated by the "Therapists Toolkit" from www.neuroinnovations.com.
Probably the least utilised facility (that is provided by current software solutions) is the ability to make use of multi media in the form of background images, tracking object images, background sounds and background voice audio. Although least utilised these features are probably the most likely to leverage greater levels of change from established EMDR protocols and EMDR therapy generally.
Computer based eye movement therapy (EMDR) usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
NLP - Neuro Linguistic Programming
Neuro Linguistic Programming (NLP) can be defined as a method and philosophy to explain the processes behind human thoughts and behaviours, as well as a large collection of psychotherapeutic tools to change thoughts and behaviours.
NLP was co-founded by Richard Bandler and John Grinder in the 1970s. They researched how successful psychotherapists such as Virginia Satir, Milton Erickson and Fritz Perls were able to generate positive therapeutic results. As a result of this research Bandler and Grinder were able to model and combine these processes into a new form of psychotherapy. [Ref]
"NLP is a study of Human Excellence that leaves behind it a trail of tools and techniques" (a quote said to have been made by Richard Bandler)".
It is that "trail of tools and techniques" that computers in particular can help to automate and bring alive. Many of the techniques are relatively visual and can be quite complex for the therapist to explain and for the patient to understand. Perhaps because of this, it is sometimes said that NLP techniques work best with those that have attended some form of NLP training!
The most frequently used NLP techniques include:
- The Map Across technique (sometimes referred to as sub modality mapping or transfer)
- The Swish Technique
- NLP Anchoring (a method of generating or collapsing conditioned responses)
- Fast Phobia Technique (cinema desensitisation / dissociation technique / rewind technique)
(A possible criticism of any computerised version of any NLP technique is that it potentially prevents the patient from accessing and developing their powers of visualisation and imagination. This downside must however be balanced against the substantial time savings of being able to visually demonstrate the technique to the patient).
The Map Across technique
The Map Across technique maps the modalities of something that is eg liked into the modalities of something that is eg disliked. A modality could be an associated feeling, image, or sound. When something that is disliked is mapped into something that is liked the effect is aversive. (See section on aversion). When the approach is reverse the technique can be used to undo aversive responses.
Computer based methods of demonstrating the Map Across technique have been on the market for some time now. One example is the aversive set of products available from www.neuroinnovations.com [Ref] [Ref]
As with all aversive techniques substantial client buy in is required, the effect may be short lived, it is possible to become desensitised to aversive stimuli during the course of therapy and some people may be highly desensitised to aversive stimuli from the outset.
The Swish Technique
The Swish technique is can be used as an alternative to the Map Across technique and also tends to map the sub modalities of one thing into another. The method is quite visually dynamic and involves images moving from left to right and from the foreground to the horizon and back again. Consequently the Swish technique in particular can benefit from computerisation at very least to explain the convoluted process to the patient. [Ref]
 The "NLP Swish" product from www.neuroinnovations.com guides the user step by step through the visualisation process and ensures that the correct eye movements are being generated.
The "NLP Swish" product from www.neuroinnovations.com guides the user step by step through the visualisation process and ensures that the correct eye movements are being generated.
Optionally the use can specify their own images (lite and pro versions) and sounds (pro version only) to customise the process to the individual.
The software is an interactive animation in the case of the lite version and a full stand-alone application in the case of the pro version.
NLP Anchoring
NLP anchoring is a powerful and very kinaesthetic and involves a specific feeling being conditioned or strongly associated with a cue such as a word or two fingers being pressed together. It is most commonly used to condition strong resourceful feelings such as confidence, strength, happiness and even aversive responses. The stimulus response cycle has to be repeated very many times in order for the response to be sufficiently conditioned. A product was in development by www.neuroinnovations.com covering NLP anchoring at the time of writing, Other software based solutions were not identified. There were some DVD and video based resources available. [Ref]
Fast Phobia Technique
The NLP "Fast Phobia Technique (Cure)" is a dissociative method that has been used to treat phobias and traumatic past experiences.
The process involves imagining sitting in the middle of a cinema and seeing on the cinema screen an image of one's self. The patient then floats up to the projection booth where they can see themselves sitting in the middle of the cinema and also see themselves projected as a still image on the cinema's screen. They then play the eg traumatic memory as a black and white movie at normal speed. Then they step into the image on the screen and turn the movie into a full colour move and rewind it very quickly back to the beginning such that they experience everything happening in reverse. Finally they float back to the projection booth and the therapist asks them to rank their current level of disturbance when thinking about the memory on a SUDS scale. [Ref]
A variety of audio and DVD / video based products are available to demonstrate the technique to patients in advance of actioning the process in the imagination. It is probably very important that the patient actions the process in their imagination in order for therapeutic change to occur. [Ref] [Ref]
An animated interactive method of demonstrating the Fast Phobia Technique was in development by www.neuroinnovations.com at the time of writing. Other software based solutions were not identified.
NLP Coaching
 NLP coaching typically calls upon NLP meta-modelling questioning combined with many NLP techniques and a generally solution or goal focused approach. Although easily automated market demand has been insufficient to justify a full stand-alone application. A stand alone application was developed and released by www.changemechanics.com in 2004 but was withdrawn from the market due to lack of demand a web based version of the product was available for some time afterwards but also appears to have been abandoned. (See screen shot above).
NLP coaching typically calls upon NLP meta-modelling questioning combined with many NLP techniques and a generally solution or goal focused approach. Although easily automated market demand has been insufficient to justify a full stand-alone application. A stand alone application was developed and released by www.changemechanics.com in 2004 but was withdrawn from the market due to lack of demand a web based version of the product was available for some time afterwards but also appears to have been abandoned. (See screen shot above).
Other attempts to automate meta model questioning were also developed at around the same time eg by neuroinnovations.com but were also abandoned. [Ref]
 The "NLP Coach" from www.nlpcoach.uk.net is deigned as an NLP practice tool for use by therapists for use on themselves. It hones the therapist's skills by providing and large range of simulated conversational scenarios.
The "NLP Coach" from www.nlpcoach.uk.net is deigned as an NLP practice tool for use by therapists for use on themselves. It hones the therapist's skills by providing and large range of simulated conversational scenarios.
Use by patients is limited and not the intended audience or market.
The Future
It is probable that NLP meta modelling style questioning patterns will be quietly merged into interactive counselling and guidance systems because the language patterns are so predictable and can be very subtle.
NLP as a movement has is probably now had its day and interest does appear to be reducing over time. This will have an impact on demand and the willingness of developers to invest in a small and receding market. A resurgence of interest could change this situation.
Computer based Neuro Linguistic Programming (NLP) usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
TFT - Thought Field Therapy
Thought Field Therapy is an unusual psychotherapeutic technique developed by American psychologist Roger Callahan. The process involves tapping on various meridian points in a specific order. The tapping sequence is referred to as an algorithm. A number of algorithms have been developed to treat different issues including anxiety, depression and trauma. [Ref] [Ref]
Because the tapping sequence can be quite complex it may be advantageous to use a computer to guide the user through the algorithm telling them where to tap and how many times to tap. If the technique works only because of distraction and the engagement of logical mental processes then computerisation could be disadvantageous. If the process works as claimed then the reverse would be true. [Ref]
 "Dynamic TFT" from www.neuroinnovations.com visually guides the user through the Thought Field Therapy process to relieve anxiety. The stand alone application is interactive and the user is asked to rank their level of anxiety at various stages on a SUDS scale.
"Dynamic TFT" from www.neuroinnovations.com visually guides the user through the Thought Field Therapy process to relieve anxiety. The stand alone application is interactive and the user is asked to rank their level of anxiety at various stages on a SUDS scale.
No other software products were identified. Simple audio CDs and DVDs may be available.
The Future
Market demand for TFT software is thought to be very minimal. Thought Field Therapy techniques may however become integrated into other products.
Computer based Thought Field Therapy usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
Low Frequency Audio
When we are exposed to low and very low frequency sounds there appears to be a direct psychological effect. Different frequencies seem to generate different effects: [Ref]
- Beta 40 - 13Hz = Alert and mentally active
- Alpha 12 - 8Hz = Relaxed
- Theta 7 - 4Hz = Deep relaxation or meditation
- Delta 4 - 0.1Hz: = Very deeply relaxed or deep sleep
It is however very difficult to generate these frequencies using standard audio equipment such as CD player stereo systems or computers. A typical sound card in a computer can generate sound that is eg 30 Hz or higher, speakers and headphones can have low frequency thresholds of eg 48 Hz. This means that if the speakers cannot generate sounds that are lower than 48 Hz a CD containing low frequency audio sounds would be totally silent. [Ref] To directly generate these low frequencies requires specialised equipment. [Ref]
To circumvent this technical limitation an approach was developed that generated the same effect, but that used audible sound. The sound is generated by the brain itself when different tones are played to each ear at the same time. The strength of the tone is varied at a low frequency (known as amplitude modulation) and low frequency sound is perceived as a pulse or beat. This effect is known as "binaural beats". [Ref] [Ref]
"If a pure tone of 400 Hz is presented to the right ear and a pure tone of 410 Hz is presented simultaneously to the left ear, an amplitude modulated standing wave of 10 Hz, the difference between the two tones, is experienced as the two wave forms mesh in and out of phase within the superior olivary nuclei".
A related concept is that of brainwave entrainment which involves generating binaural beats that gradually change their frequency over time. Brainwave patterns seems to follow the frequency as it changes if the level of change is slow enough. Typical uses are to generate relaxation in which case the frequency might start at 40 Hz (alert) and descend 20 4 Hz (deeply relaxed). [Ref]
Binaural beats audio can be used by hypnotherapists as background audio, for self hypnosis purposes, for meditation and to mask other sounds.
A number of software products have been developed that generate binaural beats and enable brainwave entrainment:
 "GNaural" from gnaural.sourceforge.net is a freeware (open-source) software product designed to allow the user to build their own entrainment audio. Some presets are available such as "meditation" or "study" but are not part of the installation. [Ref]
"GNaural" from gnaural.sourceforge.net is a freeware (open-source) software product designed to allow the user to build their own entrainment audio. Some presets are available such as "meditation" or "study" but are not part of the installation. [Ref]
In comparison with the eg Neuro Programmer the sound is slightly harsher and more difficult to listen to unless the sound is merged into eg music as recommended by the developers.
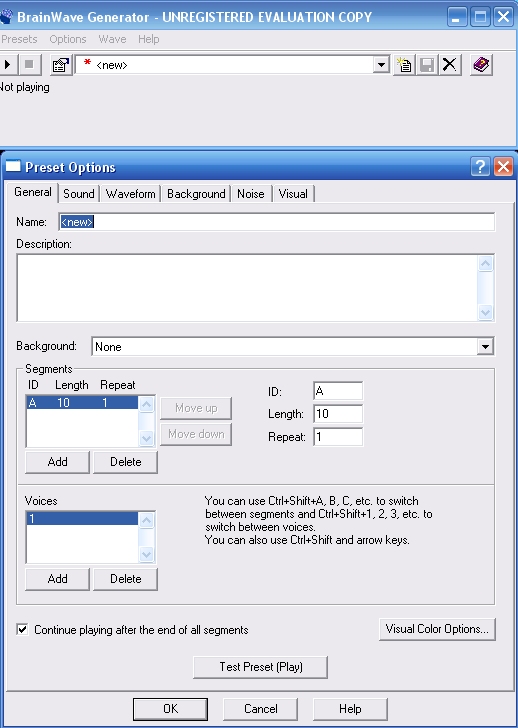 "bwgen" or Brainwave Generator from www.bwgen.com is a low cost shareware software product designed to allow the user to build their own entrainment audio. A number of presets are built-in which means that the product is immediately usable. [Ref]
"bwgen" or Brainwave Generator from www.bwgen.com is a low cost shareware software product designed to allow the user to build their own entrainment audio. A number of presets are built-in which means that the product is immediately usable. [Ref]
The sound produced was software than generated by GNAural and installation was easier than was the case with GNAural.
The overall design is suitable for novice computer users and help windows guide new users through the process of using the system.
A session editor is also present but can be difficult to use. This is true of all of the session editors reviewed and simply reflects the learning curve associated the relatively technical task of generating sessions in the first instance.
This product also enables the user to easily incorporate hypnotherapeutic audio from within the product itself.
Binaural beat audio is not for everyone and a session that would result in deep relaxation for one person can have no effect on another. This may in part be because of the quality of the audio equipment being used. High quality headphones tend to generate the best effects for the greatest number of people. However, when binaural audio works it does appear to be effective.
The Future
It is probable that speaker technology will become better at reproducing low frequencies. Sub-woofers have already pushed the low frequency boundary down to around 20 Hz. [Ref] This trend is likely to continue as sound cards and multi-media sounds systems evolve. This evolution will be driven by the gaming and home cinema markets. When low frequency audio "sound" can be generated directly, and at reasonable cost, a new era of therapeutic solutions will probably evolve. [Ref] [Ref]
Computer based low frequency audio usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
Bio feedback and neuro feedback
Biofeedback can be defined as collection of technologies that enable a person to see or hear internal biological functions such as the heart rate in real-time. Neuro feedback allows a person to see or hear brain or neurological activity in real-time. Real time simply means that the feedback is provided as the biological response is being measured. [Ref] [Ref]
The bodily processes that are frequently measured are:
- heart rate directly
- heart rate variability
- skin temperature
- galvanic skin response (sweating)
- blood pressure
- overall body temperature
- muscle tension
- electrical brain activity
- heat generated by the brain
Bio and neuro feedback helps a patient to see psychotherapeutic techniques in action and can prove to them that they are in control and that the techniques do work. Bio feedback is most useful when working with stress and stress related issues, or issues that are complicated by stress including depression and hypertension.
Current solutions can be divided into two broad categories:
- Stand alone devices
- Devices that are connected to a computer
Stand alone devices
The simplest and earliest form of handheld biofeedback was in the form of stress-dot cards. Stress dots are strips of liquid crystal that change colour depending on how much heat they are exposed to. The same principle is used by some home thermometers. To test your level of stress you simply thumb over the dot and wait for a few seconds. When you release your finger the dot will have changed colour, by comparing the colour against a key you can tell how stressed (or hot/cold) you are. [Ref]
More sophisticated electronic devices measure biological functions such as heart rate and skin resistance. There are a number of advantages to hand held devices over and above portability and cost. These include the positive benefit of not needing to rely on a computer in order to see results.
There is an enormous variety of such products. A few examples include:
 One of the first handheld devices made available to the general public was the GRS2. The GRS2 measures Galvanic Skin Response by resting two fingers on sensing plates. This measures the resistance between the two fingers and therefore the amount of perspiration. In turn this can provide an indication of stress levels. [Ref]
One of the first handheld devices made available to the general public was the GRS2. The GRS2 measures Galvanic Skin Response by resting two fingers on sensing plates. This measures the resistance between the two fingers and therefore the amount of perspiration. In turn this can provide an indication of stress levels. [Ref]
(Unusually for hand-held devices there is also the option to use the GRS2 with software so that result can be displayed in real time on a computer screen via their "CalmLink" software package. [Ref]
 "EM Wave" from www.toolsforwellness.com is a handheld stand alone device that measures heart rate variability and displays results via an LED display and via sounds. It is suitable for use self use and can be used by therapists when working with patients. [Ref]
"EM Wave" from www.toolsforwellness.com is a handheld stand alone device that measures heart rate variability and displays results via an LED display and via sounds. It is suitable for use self use and can be used by therapists when working with patients. [Ref]
Devices that are connected to a computer
Computer connected devices are somewhat more sophisticated than their hand held equivalents. A notable issue with this type of product is that compatibility and data capture issues means that they can be difficult to use.
There a many products designed for this purpose. They include:
 Calmlink from webideas.com is a biofeedback software and sensor package. The sensor measure Galvanic Skin Response and the computer software displays results on a computer screen. The connection between the device and the computer is via fibre optic cable which means that electrocution is impossible and data transfer problems are greatly reduced. [Ref]
Calmlink from webideas.com is a biofeedback software and sensor package. The sensor measure Galvanic Skin Response and the computer software displays results on a computer screen. The connection between the device and the computer is via fibre optic cable which means that electrocution is impossible and data transfer problems are greatly reduced. [Ref]
 Healing Rhythms is a computer based biofeedback device from www.toolsforwellness.com It includes a finger sensor that measures skin conductivity levels and heart rate variability, as well as software to display readings on a computer screen.
Healing Rhythms is a computer based biofeedback device from www.toolsforwellness.com It includes a finger sensor that measures skin conductivity levels and heart rate variability, as well as software to display readings on a computer screen.
Comprehensive instructions covering guided meditation and breathing exercises are also part of the package.
Healing Rhythms is an expansion of a product called "Wild Divine". Wild Divine turns the concept of biofeedback into an interactive game whereby the more relaxed a person becomes (and stays) the further they progress through the game. [Ref]
Neuro feedback is currently very expensive and is certainly not a feasible solution for the use of the general public. Several electrodes have to placed carefully around the head and a conductive gel must be applied in between the sensors and the skin. This means that practical problems such as the amount of time required to connect sensors to the scalp can emerge. As a result it is difficult to see how neuro feedback could be utilised within a busy psychotherapy practice where time is money. Another issue associated with Neuro feedback is the high level of skill required in order to interpret results in a meaningful way. There are however a few exceptions including Neurobit Lite (below).
 Neuro Bit Lite from www.neurobitsystems.com is an affordable, usable EEG neuro feedback software and hardware system. It is suitable for use by those not trained in neuro feedback analytical and diagnostic techniques ie the general public and most psychotherapists. The cost is approx $1,000 USD including the software to display results on a computer screen. Connection to a computer is optional meaning that the device could be used when travelling away from base. [Ref]
Neuro Bit Lite from www.neurobitsystems.com is an affordable, usable EEG neuro feedback software and hardware system. It is suitable for use by those not trained in neuro feedback analytical and diagnostic techniques ie the general public and most psychotherapists. The cost is approx $1,000 USD including the software to display results on a computer screen. Connection to a computer is optional meaning that the device could be used when travelling away from base. [Ref]
Hemoencephalography may bridge the gap by measuring neurological activity by shining an infrared beam through the head. This can be achieved by using emitters and sensors that can be placed lightly around the head. The costs of HEG machines is still high and machines tend to be almost hand built to order. [Ref] [Ref]
The Future
As biofeedback and neuro feedback technologies evolve it is probable that they will become smaller, cheaper and easier to use. This will be most true of neuro feedback devices that are currently difficult to use and can be very expensive. This is in the main because such technologies do not receive the level of investment that would be required to generate a mass produced high-street solution. If the computer gaming market latches onto biofeedback then this position will change very rapidly.
Biofeedback usage summary:
|
To treat:
|
Techniques / style:
|
Methods:
|
Conclusion - A brave new world...
Thus far we have taken a brief look at technologies that are currently in existence or that will probably become viable in the very near future. There are however forms of technology that may or may not exist at the current time, but that almost certainly will exist in the near future. Technology that is beyond the bleeding edge so to speak. Such technologies probably currently exist only in University departments and military research labs. [Ref]
Therapy rooms of the future may use powerful electro-magnetic fields to generate targeted neurological activity deep within the brain. In very literal terms this type of therapy could reach the parts that other therapies do not reach. This innovation would probably follow on from improvements in brain activity imaging that would allow a functional brain map to be generated for us all. We would all need our own functional brain maps to tell our therapists which areas of our brain were responsible for what function. With a personalised brain-map the magnetic forces could be directed to the right place despite individual variations. [Ref] [Ref]
Therapists of the future may find innovative ways of being with their clients at times of need without being physically present. Television programs have already wired patients for sound so that they can hear their therapist through a headset. Taken a few steps further therapists may use low power ultrasonic waves to provide ongoing instructions totally wirelessly. Ultrasonic waves can carry verbal suggestions that are only "audible" within the brain cavity itself. The patient would need to wear one emitter and the therapist could then broadcast to an entire room using another emitter. The patient would be the only person that could hear the sound because the intersection of the two waves would only be within them. The same approach could be used to convey messages to entire rooms. [Ref] [Ref]
A more invasive innovation would be to embed electronics within the brain itself. Surgeons have already implanted electrodes deep within the brains of severe epileptics, so the precedent has been set. Further down the line we may see embedded communications equipment for the ultimate mobile phone experience. At the touch of an ear lobe we could be able to call upon a virtual therapist for guidance or assistance. [Ref] [Ref]
More practically it is likely that therapy chairs will evolve and they too will be packed with technology as are current gaming chairs. The new era therapy chairs will be able to take real-time biofeedback measurements without needing to attach sensors. They will contain built-in infrasound transducers to flood the body with calming low frequencies and built-in speakers to avoid the therapist needing to speak too loudly. Microphones could monitor the quality of the patients intonation and alert the therapist to distress even before the patient becomes aware of it. When the therapist asks "how do you feel about that spider now on a scale of 1 to 10" they will be able to compare the given verbal response against emotional and biofeedback responses. [Ref]
When we truly value relaxation as a society there will be walk-in relaxation studios on every high street, perhaps even within most work-places. The driver for this change may be caused by a major reduction in flying as massive environmental taxes make flying a luxury rather than the norm. If this were the case we would be more motivated to seek relaxation closer to home.
It is also probably true that computers will increasingly become the front-line providers of automated initial response health services. Arguably the Internet is already serving that purpose to some extent. The future may see diagnostic booths in every GP surgery with a computer taking basic biological readings, asking questions, analysing responses and providing medical and psychological advice. The computer would then refer the case to an appropriate human practitioner as required.
Computer assisted psychotherapy may even become a psychotherapeutic field in its own right. Computer therapy would need to be totally eclectic and draw upon techniques from every field of psychology, psychiatry and psychotherapy. Because of this it could rise above the field based boundaries that human therapists are prone to. The computer based approach will be psychotherapy in the true sense of the word. That means no field boundaries. No personal preferences. No allegiances to a particular school of thought. Just the right combination of techniques for the right person at the right time, depending on the nature of the issue and the beliefs and values of the person in front of the screen. [Ref] [Ref]
Back to reality...
In the real world, although some of the revolutionary changes mentioned above will probably happen one way or another, the evolution will be gradual and incremental.
The reality is that by far the majority of therapists would probably class themselves as computer novices and techno phobes. This implicitly restricts the available market for software and devices for use by psychotherapists, which in turn reduces the amount of investment in these newer technologies and greatly restricts the marketing spend when releasing new products, which means that demand is not stimulated. This is the cycle for an emerging market. The cycle is broken when cluster of innovations become "must have" items. This would motivates therapists to overcome their fears of technology and jump on board because most other therapists are doing so. This generates a cascade of demand and be led by therapists or by the general public.
The general public at large represents a vast market. There are more than six and a half billion of us and about one billion computers. Products that appeal to the general public and that can also be used by therapists are likely to attract the attentions of serious investors. Serious investors are the major corporations of the world such as Microsoft and EA. If they feel that a market can be developed they have the money to re-engineer an all-new world-beating solution. If they need to, they have the power to simply buy-out smaller companies that might compete against their super-product, or that might contain some innovation that they want. It is interesting to note that games producers (eg Nintendo DS) have already begun to target the adult mind-development market by releasing hand-held devices to improve mental skills! [Ref]
Computer assisted psychotherapy and mind-changing products are here to stay. There will come a time when they will be as commonplace within every home as televisions. They will and are increasingly becoming an integral part of the technological infrastructure that we surround ourselves with. So next time you collapse on your sofa complaining of a bad day a pleasant voice from the screen in the corner of the room might just say "I hear you saying that you've day could have been better... Tell me more I wonder how you can just let those feelings go and allow yourself to relax... How would you have liked your day to have been?"
©Bill Frost 2007 BSc(Hons), PDCHyp, MBSCH
Appendices
Declaration of interests
I am affiliated with the following website:
- www.neuroinnovations.com - technology for psychotherapists
- www.changingstates.com - provision of psychotherapy via EMDR, NLP and clinical hypnotherapy
- www.transparentcorp.com - affiliate membership (I receive a conceptual comission on sales via links on my websites)
I mention products owned by Neuro Innovations throughout this document only because the primary purpose of Neuro Innovations is to generate this type of software. In all cases where other products have been identifiable they have been listed even if by doing so would involve mentioning a competitor.
Ethical Considerations
When considering computer and technology enhanced or assisted psychotherapy a number of ethical considerations apply to therapists, technology developers and patients or users of that technology. Some of those considerations apply equally to self help resources such as books. [Ref] [Ref] [Ref] [Ref]
Issues for the therapists and their patients
Therapists should consider the suitability of a patient before suggesting the use of a particular technical resource. Aspects to consider might include?
- Does the therapist or patient have the technical capability to use the resource?
- Does the therapist or patient fear technology?
- Does the patient need the "human" factor, the physical presence and support of a therapist?
- Does the patient have the motivation required to use the suggested resource in a consistent manner?
- What are the risks associated with the technology? Is there a risk of psychological dependence?
- Are there locus of control issues that may be compounded by using yet another external entity to change mood states? (Particularly an issue with substance abuse)
- Does the patient have the cognitive ability to utilise or comprehend the resource?
- Are there confidentiality issues?
- Is there a reluctance on the part of private therapists to use newer technologies because that might reduce the number of sessions required which would reduce the therapists overall income?
- Is there a strong advantage for therapists to use newer technologies because that would improve success rates and hence increase the number of patients that they are able to treat?
Issues for developers
- To what extent can access to resources be controlled?
- Are there measures in place to identify who has used the resources over time?
- Are there measures in place to limit liability - especially in the case of misuse?
- Is onward distribution by the user to their friends controlled?
- Is there a process of patient evaluation in place to determine suitability for the product?
- How is service continuity ensured?
- How is self-diagnosis mitigated?
- Should access to the resource be open or closed (freely available versus available only via a GP)
- Is it ethically justifiable to charge for access to the resource (setting business constraints to one side)?
- Is payment for access to the resource beneficial in order to increase motivation to use the resource and value for the resource?
- Is the technology mature enough for release?
- Is there research available to support the efficacy of either the technology itself or the psychological technique being employed?
- Is the resource sufficiently adaptable to individual needs of therapists or their patients?
- Is the physical presence of a therapist required in order for the therapeutic technique to be effective?
- How are issues of patient dependence mitigated? I this a developer's responsibility?
- Does the technology generate too much of an external locus of control? How is this managed?
Literature review
To some extent publications to date have largely ignored the use of technology as a therapeutic tool in it's own right for use by therapists during the course of the therapeutic process. The focus of early works was on emerging technologies that were at the time of publication "emergent" such as video conferencing and eMail. This expanded to incorporate the use of the internet for the distributed provision of self help resources and the use of computers as a means of collecting and evaluating psychometric data.
The following sources were identified:
Technology in psychotherapy: an introduction.
Newman MG.
J Clin Psychol. 2004 Feb;60(2):141-5
On the technology of psychotherapy.
Strupp HH.
Arch Gen Psychiatry. 1972 Mar;26(3):270-8.
[Book] Technology in Counselling and Psychotherapy: A Practitioner's Guide
S Goss, K Anthony - 2003
Palgrave Macmillan
Commentary: Computer-Based Interventions in Paediatric Psychology
Journal of Paediatric Psychology 29(4) pp. 269-272, 2004
New and Old Tools in Psychotherapy: The Use of Technology for the Integration of Traditional Clinical Treatments
Castelnuovo, G. Gaggioli, A. Mantovani, F. Riva, G.
PSYCHOTHERAPY -RIVER EDGE- 2003, VOL 40; PART 1/2, pages 33-44
Manual-guided cognitive-behavioral therapy training: a promising method for disseminating empirically supported substance abuse treatments to the practice community.
Morgenstern J, Morgan TJ, McCrady BS, Keller DS, Carroll KM.
Psychol Addict Behav. 2001 Jun;15(2):83-8.
Computer Based Psychotherapy for Treatment of Depression and Anxiety
14th Annual IEEE International Conference and Workshops on the Engineering of
Purves
Computer-Based Systems (ECBS'07) pp. 334-338
Computer- and internet-based psychotherapy interventions
Taylor, C. Barr; Luce, Kristine H.
Current Directions in Psychological Science, Volume 12, Number 1, February 2003 , pp. 18-22(5)
Multimedia Technology Defined
DVD
The standard interactive DVD format allows for limited interaction sufficient to allow a use to navigate through a small network of video clips. Textual material titles / instructions etc is converted into video format and is treated as another video clip in the network. Interaction is typically limited to "move cursor" and "click". This type of DVD can be played in a standard DVD player or via a computer.
DVDs designed for use with computers only have greater potentials for interaction including the ability to enter textual responses and to record those responses to the user's hard-drive. [Ref]
Another option uses a DVD as a local resource that is called up by a website. This obviates problems associated with broadband speed that greatly affect video via the internet. This method of using a DVD is known as a "web enabled DVD". [Ref]
Web / Internet
Websites can be made interactive by the use of programming languages such as JavaScript, PHP, Perl, VBScript, Flash and ASP (to name but a few). They allow for considerable interaction and Flash in particular is an excellent (although complex) web animation tool. [Ref]
Stand Alone Application Programming
There is a wide variety of programming languages that are suitable for the development of stand-alone interactive applications. Such applications are designed to run on a personal computer. (Code that runs within a internet browser or on an internet server is a web based distributed application). [Ref]
Gaming Consoles
Gaming consoles are considerably more advanced than used to be the case. They are now in effect custom computers that have been optimised for multi media gaming use. Applications have to be custom build for each major console on the market which can be a costly process. [Ref]
Virtual Reality
Full scale Virtual Reality systems combine custom video hardware in the form of headsets with motion simulation technology to emulate reality and high spec computers. The technology is reducing in price but is till relatively costly. VR systems are also technically very complex and can be prone to failure. User interaction is via movement sensors in the headset or in gloves worn by the user. [Ref]
Artificial Intelligence
Artificial Intelligence systems are improving and are generally used to make "intelligent guesses" to improve interaction within other, more conventional, systems. Use of AI systems within psychotherapy is relatively limited at the time of writing. [Ref]
See also Natural Language Processing (NLP) below
Natural Language Processing (NLP)
Natural Language Processing scripting languages enable a user to communicate naturally and for that communication to be "understood" or processed by the computer. This allows the computer to analyse eg a question and to query a database on the basis of its understanding of that question in order to provide relevant answers. NLP also allows for the generation of audio that appears natural even through it is computer generated. [Ref]
See also speech recognition [Ref]
Keywords
Images
Tables
Bibliography / References
Misc resources
- http://www.psychology.org/links/Resources/Software/
- http://www.medgadget.com/archives/psychiatry/
- http://www.bruceeisner.com/mindware/
- http://www.toolsforwellness.com/
- http://www.toolsforwellness.com/63041.html
Word Count
Last Updated 21 June 2026 © www.neuroinnovations.com 1998-2023
|
|